
In the summer of 2016, I worked in a team at Bihar Innovation Labs to research and solve issues in the healthcare sector.
We’ve been covering Economic Development in school this semester, which I felt tied in with the project I worked on.
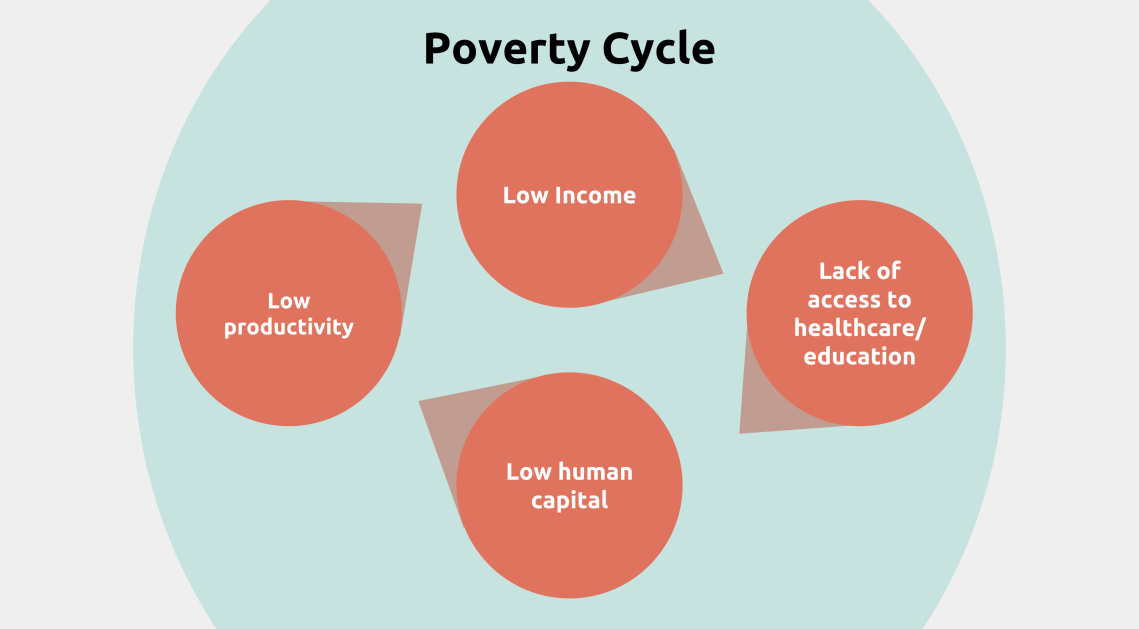
There are many arguments that argue the poverty cycle does not exist. But for now, let’s assume it does.
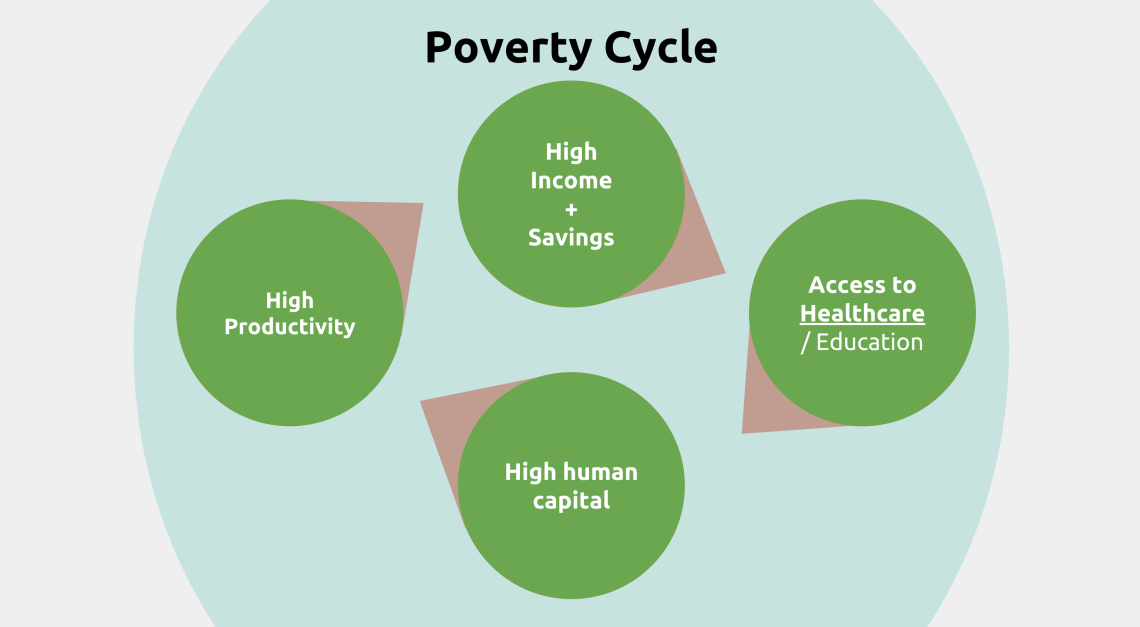
The premise of escaping the poverty cycle goes as follows: by providing healthcare, human capital can be increased, resulting in higher productivity, which makes individuals more desirable in the labor market or more productive in the fields. Higher productivity leads to higher income, and families can escape the poverty cycle.
It seems simple, but it isn’t.

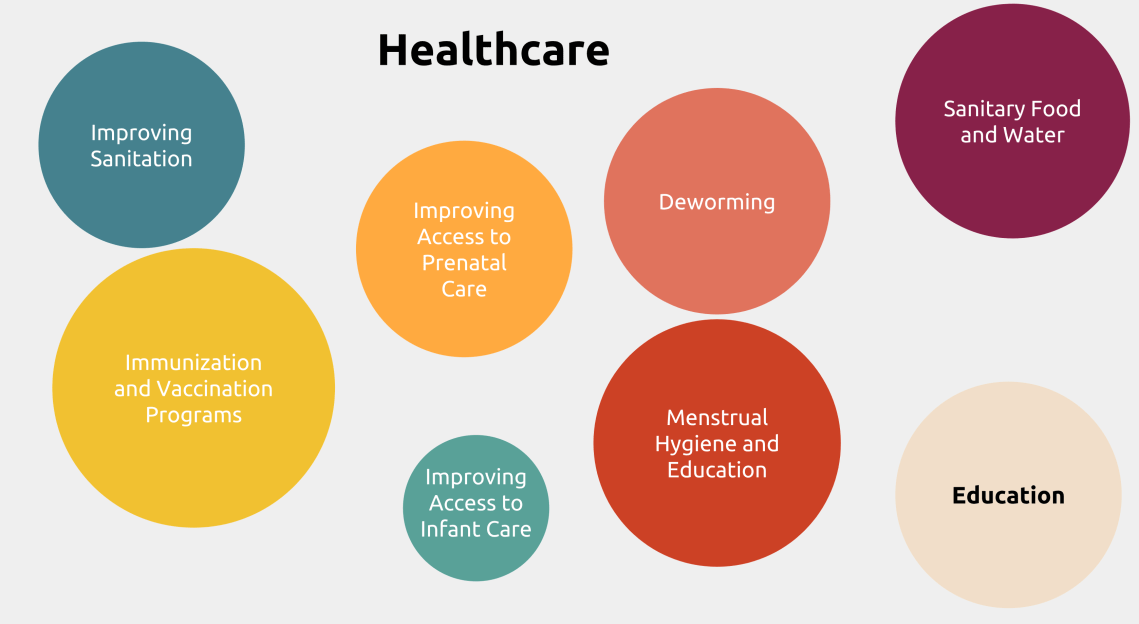
“Poor Economics” author Abhijit Bannerjea describes “low hanging fruit” as the easy answer to development challenges. Things like deworming medicine, ORS for diarrhea, immunizations are all easy answers to major problems facing healthcare sectors in LEDCs, but picking this low hanging fruit is not as easy as it seems. When healthcare infrastructure exists ( no matter how poor), there are thousands of families that still are unable to take advantage of the existing ecosystem of healthcare. Take immunizations for example:
Obviously, immunizations are good. Obviously, we should get immunizations to the people. And obviously, the government is trying to immunize citizens. So then why do so many people not get immunized? Why is access still undependable, and what last mile problems are preventing care from reaching people?
Throwing money at solving these problems isn’t the solution either. In order to truly pick low hanging fruit, I appreciated the approach I learned at Bihar Innovation Labs, where we used innovation and product design to tackle challenges based on intensive research.
The Process:

The first step involved going to the field for months and immersing ourselves in the ecosystem. This meant following healthcare workers on their immunization runs and routines, interviewing hundreds of mothers, and generally soaking up information around us.
We then came back to the lab with stacks of “problem cards” that condensed our insights down into tangible problems we wanted to solve. This ranged from “bottle labels are illegible” to “mothers feed expired medicines to children” to even “family planning programs conflicts with Islamic ideologies”.
To begin solving these issues, we sat around a table with hundreds of sticky notes and cards to brainstorm together. At this stage, any idea was a good idea, nothing was refuted, and nothing was too wild. We made sure to tie our solution to specific insights from the field when applicable.

Eventually, we rapid prototyped a few ideas to validate concepts, refined ideas, and selected a few projects to carry forward. Then the cycle would repeat, with the added element of testing these projects with the users.

Some background on Bihar’s healthcare ecosystem:
There were two government aid workers that a majority of our research centered around: ASHAs and Anganwadis. Furthermore, some of the villages had Primary Healthcare Centers (PHCs) – clinics that are two levels down from a hospital. Some villages were lucky to have these, but scaling them to every village had proved to be an unsustainable goal for the government.
The problem spheres in this ecosystem are so nuanced and no easy solution exists. And then there’s the fact that education and healthcare are intrinsically linked. With better education arises better healthcare. Encouraging behavioral change is easier when people believe that solutions work. But changing beliefs is much harder than encouraging better habits. Here are two of the problems we focused in on.
Problem: Immunization runs are difficult for ASHAs
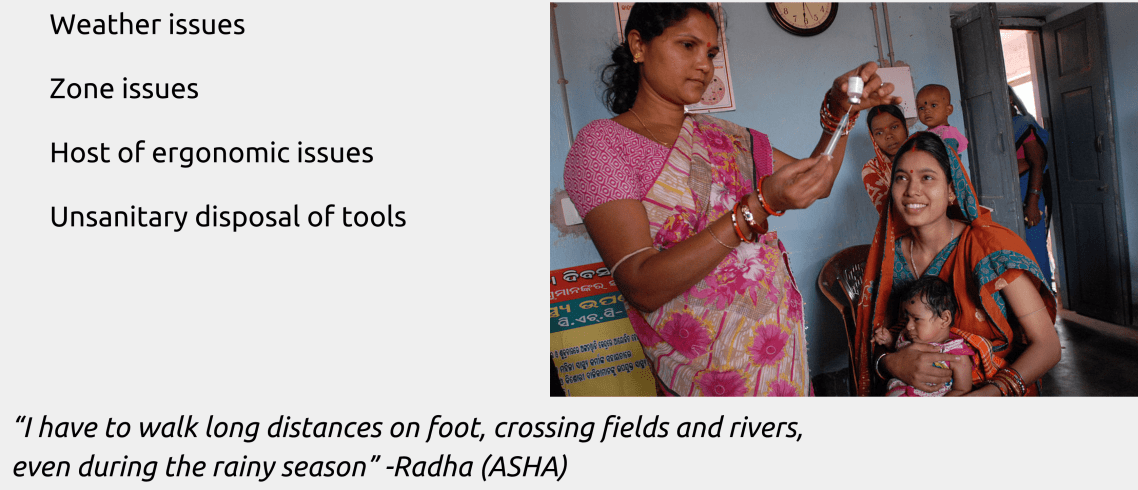
Solution: A redesigned medical backpack that turns into a workstation

Specific features:


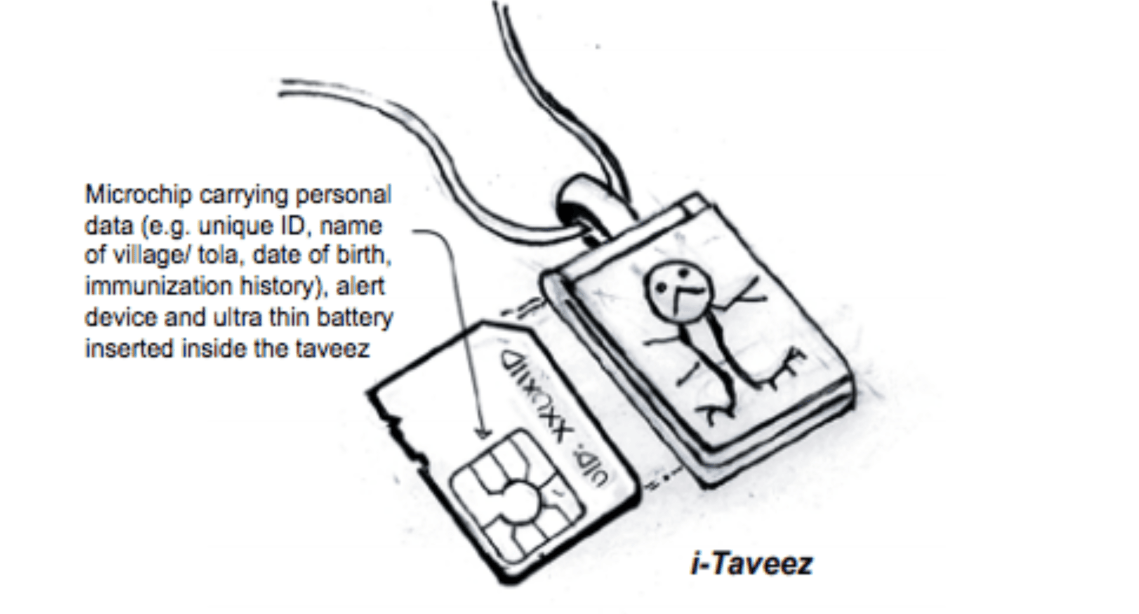
Problem: Physical records get misplaced, are incorrectly filled or don’t exist.

Note the problem was especially pronounced because most workers and mothers could not read the Hindi that was used on these forms.
Solution: iTaweez. Repurposing Taweez (a spiritual charm given to every newborn in villages) as a database for a child’s immunization records

I end with some questions to consider:
- Is spending more on healthcare the solution to development challenges?
- How can we use behavioral economics (e.g. nudge theory) to understand situations and design better policies
- There is no silver bullet. Nuanced problems require nuanced solutions. How can these solutions be scaled then?
